

Coronary artery disease
Highlights
Coronary Artery Disease
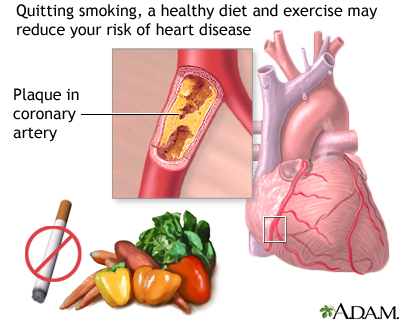
Coronary artery disease (CAD), also called heart disease, is a condition in which fatty deposits called plaque build-up in the heart’s arteries. These deposits cause arteries to become narrow and blocked, which restricts blood and oxygen flow to the heart muscle. CAD is the leading cause of death, for both men and women, in the United States.
Risk Factors
The most important factors that increase the risk for CAD are:
- Smoking
- Unhealthy cholesterol and lipid levels
- High blood pressure
- Diabetes
- Lack of exercise
- Obesity
- Advancing age
Symptoms
Angina is the primary symptom of coronary artery disease. Angina feels like gripping pain or pressure in the chest area.
- Stable angina is predictable chest pain that lasts a few minutes or less and is usually relieved by rest or medication. It is often triggered by physical exertion or emotional stress.
- Unstable angina is unpredictable chest pain that occurs unexpectedly, even when at rest. It is a more serious condition than stable angina and can be a warning sign of a heart attack.
Some patients with CAD have few or no symptoms. Sometimes a heart attack may be the first sign that a person has CAD.
Treatment
- Lifestyle changes (such as a healthy diet and regular physical activity) are essential for preventing and treating CAD.
- Medications for preventing and treating CAD include aspirin, cholesterol-lowering drugs (statins), and high blood pressure medications. Some patients take nitrate drugs such as nitroglycerin or other medications to treat angina.
- Procedures may be needed to open blocked or narrowed coronary artery and improve blood flow to the heart. This approach is known as reperfusion therapy. Percutaneous coronary intervention (PCI), also called angioplasty, uses a small balloon to open the blood vessel. Coronary artery bypass graft (CABG) is a more invasive procedure that is generally recommended for patients with severe heart disease. It uses grafts from arteries or veins to reroute blood flow.
New Guidelines
The American College of Cardiology, American Heart Association, and other professional organizations have released several new guidelines in the past year. Updated recommendations include:
- The guidelines emphasize the importance of blood pressure and lipid control, as well as the regular use of anti-platelet therapy (ideally aspirin) for patients with heart disease.
- Patients deciding between coronary arterty bypass graft (CABG) and percutaneous coronary intervention (PCI) should meet with an interdisciplinary medical team that includes both a cardiac surgeon and an interventional cardiologist.
- Cardiac rehabilitation is strongly recommended, especially for patients who have undergone bypass surgery. Patients who have had CAGB should also be screened for depression.
- Sexual activity is safe for most patients with stable CAD but patients with severe heart disease should abstain until their condition is stabilized.
.
Introduction
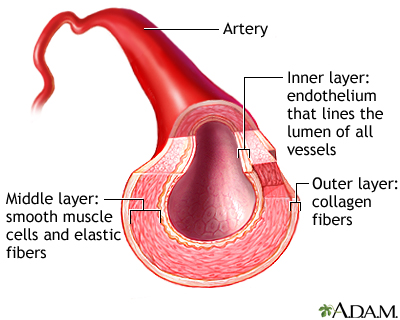
Coronary artery disease (CAD), also called heart disease or ischemic heart disease, results from a complex process known as atherosclerosis (commonly called "hardening of the arteries"). In atherosclerosis, fatty deposits (plaques) of cholesterol and other cellular waste products build up in the inner linings of the heart’s arteries. This causes blockage of arteries and prevents oxygen-rich blood from reaching the heart (ischemia). There are many steps in the process leading to atherosclerosis, some not fully understood.

Click the icon to see an image of atherosclerosis.
Cholesterol and Lipoproteins. The atherosclerosis process begins with cholesterol and sphere-shaped bodies called lipoproteins that transport cholesterol.
- Cholesterol is a substance found in all animal cells and animal-based foods. It is critical for many functions, but under certain conditions cholesterol can be harmful.
- The lipoproteins that transport cholesterol are referred to by their size. The most commonly known are low-density lipoproteins (LDL) and high density lipoproteins (HDL). LDL is often referred to as "bad" cholesterol; HDL is often called "good" cholesterol.

Click the icon to see an image of a tear in the wall of an artery.
Oxidation. The damaging process called oxidation is an important trigger of atherosclerosis:
- Oxidation is a chemical process in the body caused by the release of unstable particles known as oxygen-free radicals. It is one of the normal processes in the body, but under certain conditions (such as exposure to cigarette smoke or other environment stresses) these free radicals are overproduced.
- In excess amounts, they can be very dangerous, causing damaging inflammation and even affecting genetic material in cells.
- In heart disease, free radicals are released in artery linings and oxidize low-density lipoproteins (LDL). The oxidized LDL is the basis for cholesterol build-up on the artery walls and damage leading to heart disease.
Inflammatory Response. For the arteries to harden there must be a persistent reaction in the body that causes ongoing harm. Researchers now believe that this reaction is an immune process known as the inflammatory response.

Click the icon to see an image of inflammation.
There is growing evidence that the inflammatory response may be present not only in local plaques in single arteries but also throughout the arteries leading to the heart.
Blockage in the Arteries. Eventually the calcified (hardened) arteries become narrower (a condition known as stenosis).
- As this narrowing and hardening process continues, blood flow slows, preventing sufficient oxygen-rich blood from reaching the heart muscles.
- Such oxygen deprivation in vital cells is called ischemia. When it affects the coronary arteries, it causes injury to the tissues of the heart.
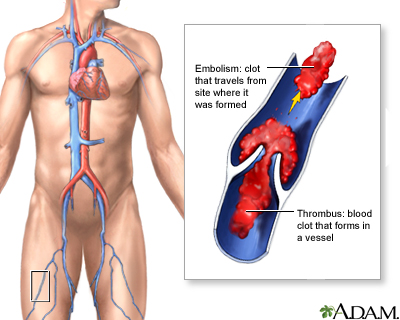
- These narrow and inelastic arteries not only slow down blood flow but also become vulnerable to injury and clot formation, which is what usually triggers a heart attack.

Click the icon to see an image of a coronary artery blockage.
The End Result: Heart Attack. A heart attack can occur as a result of one or two effects of atherosclerosis:
- The plaque itself develops fissures or tears. Blood platelets stick to the site to seal off the plaque, and a blood clot (thrombus) forms. A heart attack can then occur if the blood clot completely blocks the passage of oxygen-rich blood to the heart.
- Less commonly, the artery becomes completely blocked by plaque itself, and ischemia becomes so extensive that some oxygen-deprived muscle cells in the heart die.

Click the icon to see an image of how atherosclerosis develops.
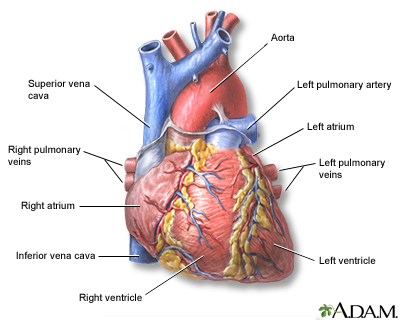

Click the icon to see an image of heart arteries.

Click the icon to see an animation of coronary artery disease.
Risk Factors
Heart disease is the leading cause of death in the United States. Over the past decades, heart disease rates declined in both men and women as they quit smoking and improved dietary habits. This improvement, however, has leveled off in recent years, most likely because of the dramatic increase in obesity in the U.S. and other industrialized nations.
Age
The risks for coronary artery disease increase with age. About 85% of people who die from heart disease are over the age of 65.
Gender
Men have a greater risk for coronary artery disease and are more likely to have heart attacks earlier in life than women. Women’s risk for heart disease increases after menopause, and they are more likely to have angina than men.
Genetic Factors and Family History
Certain genetic factors increase the likelihood of developing important risk factors such as diabetes and high blood pressure. Heart disease tends to run in families. People whose parents or siblings developed heart disease at a younger age are more likely to develop it themselves.
Race and Ethnicity
African-Americans have the highest risk of heart disease, in part due to their high rates of severe high blood pressure, as well as diabetes and obesity.

Click the icon to see an image of African-American heart disease risk.
Lifestyle Factors
Smoking. Smoking is the most important risk factor for heart disease. Smoking can cause elevated blood pressure, worsen lipids, and make platelets very sticky, raising the risk of clots. Although heavy cigarette smokers are at greatest risk, people who smoke as few as three cigarettes a day are at increased risk for blood vessel abnormalities that endanger the heart. Regular exposure to secondhand smoke also increases the risk of heart disease in nonsmokers.
Alcohol. Moderate alcohol consumption (one or two drinks a day; 5 ounces wine, 12 ounces beer, or 1.5 ounces hard liquor is one drink) can help boost HDL “good” cholesterol levels. Alcohol may also prevent blood clots and inflammation. By contrast, heavy drinking harms the heart. In fact, heart disease is the leading cause of death in alcoholics.
Diet. Diet plays an important role in the health of the heart, especially in controlling dietary sources of cholesterol and restricting salt intake that contributes to high blood pressure.
Physical Inactivity. Exercise has a number of effects that benefit the heart and circulation, including improving cholesterol and lipids, lowering blood pressure and blood sugar levels, and improving weight control. People who are sedentary are almost twice as likely to suffer heart attacks as are people who exercise regularly.
Medical Conditions
Obesity and Metabolic Syndrome. Excess body fat, especially around the waist, can increase the risk for heart disease. Obesity also increases the risk for other conditions (such as high blood pressure and diabetes) that are associated with heart disease. Obesity is particularly hazardous when it is part of the metabolic syndrome, a pre-diabetic condition that is significantly associated with heart disease. This syndrome is diagnosed when three of the following are present:
- Abdominal obesity (fat around the waist)
- Low HDL ("good") cholesterol
- High triglyceride levels
- High blood pressure
- Insulin resistance (diabetes or prediabetes)
There are numerous way to control your weight and diet.
Unhealthy Cholesterol and Lipid Levels. Low-density lipoprotein (LDL) cholesterol is the "bad" cholesterol responsible for many heart problems. Triglycerides are another type of lipid (fat molecule) that can be bad for the heart. High-density lipoprotein (HDL) cholesterol is the "good" cholesterol that helps protect against heart disease. Doctors test for a "total cholesterol" profile that includes measurements for LDL, HDL, and triglycerides. The ratio of these lipids can affect heart disease risk.

Click the icon to see an image of a blood test.
High Blood Pressure. High blood pressure (hypertension) is associated with coronary artery disease. For an adult, a normal blood pressure reading is below 120/80 mm Hg. High blood pressure is generally considered to be a blood pressure reading greater than or equal to 140 mm Hg (systolic) or greater than or equal to 90 mm Hg (diastolic). Blood pressure readings in the prehypertension category (120 - 139 systolic or 80 - 89 diastolic) indicate an increased risk for developing hypertension.

Click the icon to see an image of hypertension.
Diabetes. Diabetes, especially for people whose blood sugar levels are not well controlled, significantly increases the risk of developing heart disease. In fact, heart disease and stroke are the leading causes of death in people with diabetes. People with diabetes, both type 1and type 2, are also at risk for high blood pressure and unhealthy cholesterol levels, blood clotting problems, and impaired nerve function, all of which can damage the heart.
Peripheral Artery Disease. Peripheral artery disease (PAD) occurs when atherosclerosis affects the extremities, particularly the feet and legs. The major risk factors for heart disease and stroke are also the most important risk factors for PAD. (The combination of such conditions with PAD also produces more severe forms of heart or circulatory disease.) Even though signs of heart disease are often not evident in the majority of patients with PAD, most of these patients also have coronary artery disease.
Depression. Although people with heart disease may become depressed, this does not explain entirely the link between the two problems. Data suggest that depression itself may be a risk factor for heart disease as well as its increased severity. A number of studies indicate that depression has biologic effects on the heart, including blood clotting and heart rate. Guidelines recommend that patients who have undergone coronary artery bypass surgery or angioplasty (PCI) be screened for depression. Stress may also contribute to risk.
Risk Factors with Unclear Roles
Homocysteine and Vitamin B Deficiencies. Deficiencies in the B vitamins folate (known also as folic acid), B6, and B12 have been associated with a higher risk for heart disease in some studies. Such deficiencies produce higher blood levels of homocysteine, an amino acid that has been associated with a higher risk for heart disease, stroke, and heart failure.
However, while B vitamin supplements do help lower homocysteine levels, they appear to have no effect on heart disease outcomes, including preventing heart attack or stroke. Research indicates that homocysteine may be a marker for heart disease rather than a cause of it.

Click the icon to see an image of B vitamin supplementation.

Click the icon to see another image of B vitamin supplementation.
C-Reactive Protein. C-reactive protein (CRP) is a product of the inflammatory process. It is not known if the protein plays any causal role or whether it is simply a marker for other factors in the disease process.
C. pneumoniae and Other Infectious Organisms. Some microorganisms and viruses have been under suspicion for triggering the inflammation and damage in the arteries that contribute to heart disease. The strongest evidence to date supports a possible role from Chlamydia (C.) pneumoniae (an atypical bacterial organism that causes mild pneumonia in young adults). C. pneumoniae has been detected in plaques in the arteries of patients with heart disease. However, treatment with appropriate antibiotics has not been found to reduce the risk of future heart problems for patients infected with this organism.
Other studies suggest that cytomegalovirus (CMV), a common virus, may have similar effects. Many people, however, have been infected with these organisms, and no clear association has been found with any of these infections.
Sleep Apnea. Obstructive sleep apnea is a condition in which tissues in the upper throat sag at intervals during sleep, thereby blocking the passage of air. Patients with severe, untreated apnea are at increased risk for CAD, high blood pressure, stroke, and heart attack. However, there is no evidence to date that obstructive sleep apnea is an independent cause of cardiac events or stroke.
Periodontal Disease. Periodontal disease and heart disease are both inflammatory conditions. There appears to be an association between periodontal disease and CAD, but it is not yet clear if having one condition increases the risk of developing the other. Patients who have periodontal disease and at least one risk factor for heart disease should have a medical evaluation for heart problems. Patients who have CAD should have regular exams to check for signs of periodontal disease.
Symptoms
Common symptoms of coronary artery disease (CAD) include angina, shortness of breath (particularly during physical exertion), and rapid heartbeat. Sometimes patients with CAD have few or no symptoms until they have heart attack or heart failure.
Angina
Angina is a symptom, not a disease. It is the primary symptom of coronary artery disease and, in severe cases, of a heart attack. It is typically felt as chest pain and occurs as a consequence of a condition called myocardial ischemia. Ischemia results when the heart muscle does not get as much blood (and, as a result, as much oxygen) as it needs for a given level of work. Angina is usually referred to as one of two states:

Click the icon to see an image of agina.
- Stable Angina (which is predictable)
- Unstable Angina (which is less predictable and a sign of a more serious situation)
Angina may be experienced in different ways and can be mild, moderate, or severe. The intensity of the pain does not always relate to the severity of the medical problem. Some people may feel a crushing pain from mild ischemia, while others might feel only mild discomfort from severe ischemia.

Click the icon to see another image of angina.
Stable Angina and Chest Pain
Stable Angina. Stable angina is predictable chest pain. Although less serious than unstable angina, it can be extremely painful or uncomfortable. It is usually relieved by rest and responds well to medical treatment (typically nitroglycerin). Any event that increases oxygen demand can cause an angina attack. Some typical triggers include:
- Exercise
- Cold weather
- Emotional tension
- Large meals
Angina attacks can happen at any time during the day, but most occur between 6 a.m. and noon.
Specific symptoms that are more likely to indicate angina include:
- Angina pain or discomfort is typically described by patients as fullness or tingling, squeezing, pressure, heavy, suffocating, or griplike. It is rarely described as stabbing or burning. Changing one's position or breathing in and out does not affect the pain.
- A typical angina attack lasts minutes. If it is more fleeting or lasts for hours, it is probably not angina.
- Pain is usually in the chest under the breast bone. It often radiates to the neck, jaw, or left shoulder and arm. Less commonly, patients report symptoms that radiate to the right arm or back, or even to the upper abdomen.
- Women are particularly likely to experience atypical symptoms that often involve discomfort in the abdomen, nausea, or unusual fatigue and weakness instead of chest pain.
- Stable angina is usually relieved by rest or by taking nitroglycerin under the tongue.
Other symptoms that may indicate angina or accompany the pain or pressure in the chest include:
- Shortness of breath
- Nausea, vomiting, and cold sweats
- A feeling of indigestion or heartburn
- Unexplained fatigue (more common in women)
- Dizziness or lightheadedness
- Palpitations
Unstable Angina and Acute Coronary Syndrome
Unstable angina is a much more serious situation and is often an intermediate stage between stable angina and a heart attack, in which an artery leading to the heart (a coronary artery) becomes completely blocked. A patient is usually diagnosed with unstable angina under one or more of the following conditions:
- Pain awakens a patient or occurs during rest.
- A patient who has never experienced angina has severe or moderate pain during mild exertion (walking two level blocks or climbing one flight of stairs).
- Stable angina has progressed in severity and frequency within a 2-month period, and medications are less effective in relieving its pain.
- Fainting episode.
Unstable angina is usually discussed as part of a condition called acute coronary syndrome (ACS). ACS also includes people with a condition called NSTEMI (non ST-segment elevation myocardial infarction) -- also referred to as non-Q wave heart attack. With NSTEMI, blood tests indicate a developing heart attack. These conditions are less severe than full-blown heart attacks but may develop into major attacks without aggressive treatment.
Other Types of Angina
Prinzmetal's Angina. A third type of angina, called variant or Prinzmetal's angina, is caused by a spasm of a coronary artery. It almost always occurs when the patient is at rest. Irregular heartbeats are common, but the pain is generally relieved promptly with standard treatment.
Silent Ischemia. Some people with severe coronary artery disease do not have angina pain. This condition is known as silent ischemia, which may occur when the brain abnormally processes heart pain. This is a dangerous condition because patients have no warning signs of heart disease. Some studies suggest that people with silent ischemia have higher complication and mortality rates than those with angina pain. (Angina pain may actually protect the heart by conditioning it before a heart attack.)
Other Causes of Chest Pain or Discomfort
Chest pain is a very common symptom in the emergency room, but heart problems account for less than half of all chest pain episodes. There are many other causes of chest pain or discomfort including injured muscles, arthritis, heartburn, and asthma. Still, if you are experiencing chest pain, it is best to seek immediate medical attention.
Diagnosis
Many tests can diagnose possible heart disease. The choice of which (and how many) tests to perform depends on the patient's risk factors, history of heart problems, and current symptoms. Usually the tests begin with the simplest and may progress to more complicated ones.
Routine Tests to Determine Risk for Heart Disease
Doctors routinely check for high blood pressure and unhealthy cholesterol levels in all older adults. Specific tests are also important in people who may have risk factors or symptoms of diabetes.
Electrocardiograms (ECGs)
An electrocardiogram (ECG) measures and records the electrical activity of the heart. Up to half of people who suffer from angina or silent ischemia, however, have normal ECG readings. The waves measured by the ECG correspond to when different parts of the heart contract and relax. Specific waves seen on an ECG are named with letters:
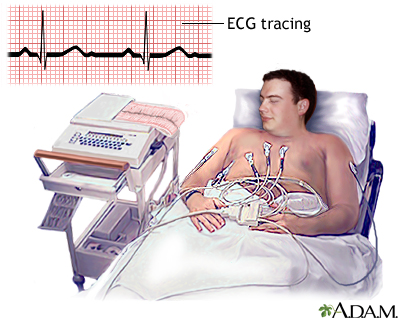
- P. The P wave is associated with the contractions of the atria (the two chambers in the heart that receive blood from outside).
- QRS. The QRS is a series of waves associated with ventricular contractions. (The ventricles are the two major pumping chambers in the heart.)
- T and U. These waves follow the ventricular contractions.
The most important wave patterns in diagnosing and determining treatment for heart disease and heart attack are called ST elevations and Q waves.
- A depressed or horizontal ST wave suggests some blockage and the presence of a heart disease, even if there is no angina present. (This wave pattern is not very accurate, particularly in women, and can occur without heart problems).
- ST elevations and Q waves are the most important wave patterns in diagnosing and determining treatment for a heart attack. They suggest that an artery to the heart is blocked, and that the full thickness of the heart muscle is damaged. ST segment elevations, however, do not always mean the patient has a heart attack. Other factors are important in making a diagnosis.
Exercise Stress Test
Exercise stress test for evaluation of coronary artery disease may be performed in the following situations:
- Patients with possible or probable angina to help determine the likelihood of coronary artery disease being present
- Patients who were previously stable who began having symptoms
- Follow-up of patients with known heart disease or after coronary bypass surgery or percutaneous procedure
- To determine a patient's functional capacity (how well the heart can respond when extra demand is needed)
- Patients with certain types of heart rhythm disturbances
- After a heart attack, either before leaving the hospital or soon afterwards
Basic Procedure. A stress test (exercise tolerance test) monitors the patient's heart rhythms, blood pressure, and clinical status. It can tell how well the heart handles work and if parts of the heart have decreased blood supply. A typical stress test involves:
- The patient walks on a treadmill or rides a stationary bicycle. Exercise continues until the heart is beating at least 85% of its maximum rate, until symptoms of heart trouble occur (changes in blood pressure, heart rhythm abnormalities, angina, and fatigue), or the patient simply wants to stop.
- For patients who cannot exercise, the doctor may administer dobutamine or arbutamine, which are drugs that simulate the stress of exercise.
An ECG is used to monitor heart rhythms during a stress test. (An echocardiogram or more advanced imaging technique may also be used to visualize the actions of the heart and blood flow.)
Interpreting Results. To accurately assess heart problems, a variety of factors are measured or monitored using the ECG and other tools during exercise. They include:
- Exercise capacity. This is a measure of a person's capacity to reach certain metabolic rates.
- ST waves on the ECG. Doctors specifically look for abnormalities in part of the wave tracing called an ST segment. A certain type of ST segment depression may suggest the presence of heart disease. However, gender, drugs, and other medical conditions can affect the ST segment.
- Heart rate. This is how fast the heart rate goes during exercise and how quickly it returns to normal recovery. Based on age and other factors, everyone's heart rate should go up to a certain level during exercise. If it does not go up to the expected level, the patient is considered at risk for heart problems.
- Changes in systolic blood pressure. Generally, the blood pressure will go up during exercise.
- Oxygen levels may also be measured.
Using these and other measures, doctors can determine risk fairly accurately, particularly for men with chronic stable angina. The test has limitations, however, and some are significant. In patients with suspected unstable angina, normal or low risk results may not be as accurate in predicting future risk of cardiac events.
About 10% of patients, particularly younger people, will have false positive test results. In such cases, test results indicate abnormalities when there are no heart problems. In addition, for many reasons, the test is less accurate in women and an echocardiogram may be a more accurate procedure for them.
Echocardiograms
An echocardiogram is a noninvasive test that uses ultrasound images of the heart. This test is more expensive than an ECG, but it can be very valuable, particularly in identifying whether there is damage to the heart muscle and the extent of heart muscle damage.
A stress echocardiogram may be performed to further evaluate abnormal findings from an exercise treadmill test or a routine echocardiogram. Examples include identifying exactly which part of the heart may be involved and quantifying how much muscle has been infected. It may be the first test done when the exercise treadmill test cannot be performed due to certain abnormal rhythms.
Radionuclide Imaging
Radionuclide procedures use imaging techniques and computer analyses to plot and detect the passage of radioactive tracers through the region of the heart. Such tracing elements are typically given intravenously. Radionuclide imaging is useful for diagnosing and determining:
- Severity of unstable angina when less expensive diagnostic approaches are unavailable or unreliable
- Severity of chronic coronary artery disease
- Success of surgeries for coronary artery disease.
- Whether a heart attack has occurred
Myocardial Perfusion (Blood Flow) Imaging Test (also called the Thallium Stress Test). This radionuclide test is typically used with an exercise stress test to determine blood flow to the heart muscles. It is a reliable measure of severe heart events. It may be useful in determining the need for angiography if CT scans have detected calcification in the arteries. About a minute before the patient is ready to stop exercising, the doctor administers a radioactive tracer into the intravenous line. (Tracers include thallium, technetium, or sestamibi.) Immediately afterwards, the patient lies down for a heart scan. If the scan detects damage, more images are taken 3 or 4 hours later. Damage due to a prior heart attack will persist when the heart scan is repeated. Injury caused by angina, however, will have resolved by that time.
Radionuclide Angiography. This is a technique for visualizing the chambers and major blood vessels of the heart. It uses an injected radioactive tracer and can be performed during exercise, at rest, or with use of stress-inducing drugs. It can help determine the severity of coronary artery disease and is an alternative to echocardiograms in certain situations.

Click the icon to see an image of the heart.

Click the icon to see an image of an MRI scan.
Angiography
Angiography is an invasive test. It is used for patients who show strong evidence for severe obstruction on stress and other tests, and for patients with acute coronary syndrome. It is required when there is a need to know the exact anatomy and disease present within the coronary arteries. A limitation of angiography is that it is not always the most occluded (narrowed) artery that causes the next heart attack. In an angiography procedure:
- A narrow tube is inserted into an artery, usually in the leg or arm, and then threaded up through the body to the coronary arteries.
- A dye is injected into the tube, and an x-ray records the flow of dye through the arteries.
- This process provides a map of the coronary circulation, revealing any blocked areas.

Click the icon to see an image of angiography.
Magnetic Resonance Angiography (MRA). MRA is a newer noninvasive imaging technique that can provide three-dimensional images of the major arteries to the heart.
Computed Tomography
Computed tomography (CT) scans may be used to evaluate coronary artery disease.
Calcium Scoring CT Scans of the Heart. These scans are used to detect calcium deposits on the arterial walls. The presence of calcium correlates well with the presence of atherosclerosis of the heart. If the calcium score is very low, a patient is unlikely to have coronary artery disease. A higher calcium score may indicate an increased risk of current and future coronary artery disease. However, the presence of calcium does not necessarily signify narrowing of the arteries that would need further immediate evaluation or treatment.
CT Angiography. CT scans may also be used to visualize the coronary arteries. When compared to invasive angiography, CT angiography is not as accurate in identifying who truly has coronary artery disease and who does not. Other types of newer CT techniques include electron beam computed tomography and multidetector computed tomography.

Click the icon to see an image of a CT scan.
Prevention
Heart disease prevention is important before and after someone is diagnosed with the condition:
- Primary prevention refers to measures that everyone should take to reduce their risk of heart disease.
- Secondary prevention refers to measures a patient already diagnosed with heart disease should take to reduce the risk of having additional heart damage. Many of these measures are similar or the same as those recommended for primary prevention.
Key prevention measures include:
- All patients should stop smoking and avoid exposure to secondhand smoke.
- Maintain cholesterol levels at appropriate levels using a heart healthy diet, exercise, and medications
- Maintain an appropriate low blood pressure level
- Maintain an active lifestyle
- Use an antiplatelet drug, such as aspirin or clopidogrel, if appropriate (see Medications section of this report)
- Manage diabetes and kidney disease when present
Smoking Cessation
Your doctor should ask about your smoking habits at every visit. Smoking is a chronic condition and often requires repeat therapy using more than one technique.
Control Cholesterol
All patients should start following a heart-healthy diet and exercise regularly, after talking to their doctors.
Patients with CAD should aim for LDL cholesterol levels of less than 100 mg/dL. (Doctors may recommend levels below 70 mg/dL for certain patients.) If patients cannot reach the LDL target through lifestyle measures, current guidelines recommend a statin drug. Statin drugs are the primary medications used for lowering LDL (“bad”) cholesterol levels.

Click the icon to see an image of cholesterol.
Manage High Blood Pressure
Keep Blood Pressure Low. People in normal health should have a blood pressure reading of 120/80 mm Hg or less. Blood pressure readings of 120/80 are considered normal, readings of 140/90 or higher indicate high blood pressure (hypertension), and readings in between the two are called pre-hypertension. Patients with CAD should aim for blood pressure readings of less than 130/80 mm Hg. If they cannot achieve this target, current guidelines recommend that they receive at least two blood pressure medications.
Manage Diabetes
All patients with diabetes should have their blood sugar (glucose) levels well managed. For most patients, a goal would be to bring HbA1c levels down to around 7%. Blood pressure goals for people with diabetes, both type 1 and type 2, are currently being reexamined. At this time, the recommended goal is to maintain blood pressure readings of 130/80 mm Hg.
Heart-Healthy Diet
Current American Heart Association (AHA) for guidelines for a heart-healthy diet recommend:
- Balance calorie intake and physical activity to achieve or maintain a healthy body weight.
- Consume a diet rich in a variety of vegetables and fruits.
- Choose whole-grain, high-fiber foods. These include fruits, vegetables, and legumes (beans). Good whole grain choices include whole wheat, oats/oatmeal, rye, barley, brown rice, buckwheat, bulgur, millet, and quinoa.
- Consume fish, especially oily fish, at least twice a week (about 8 ounces/week). Oily fish such as salmon, mackerel, and sardines are rich in the omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Consumption of these fatty acids is linked to reduced risk of sudden death and death from coronary artery disease. People with existing heart disease should consider taking daily fish oil supplements of 850 - 1,000 mg eicosapentaenoic acid (EPA) and docosahexaenoic acid (DPA).
- Limit daily intake of saturated fat (found mostly in animal products) to less than 7% of total calories, trans fat (found in hydrogenated fats, commercially baked products, and many fast foods) to less than 1% of total calories, and cholesterol (found in eggs, dairy products, meat, poultry, fish, and shellfish) to fewer than 300 mg per day. Choose lean meats and vegetable alternatives (such as soy). Select fat-free and low-fat dairy products. Grill, bake, or broil fish, meat, and skinless poultry.
- Use little or no sodium (salt) in your foods. Reducing sodium can lower blood pressure and decrease the risk of heart disease and heart failure.
- Cut down on beverages and foods that contain added sugars (corn syrups, sucrose, glucose, fructose, maltrose, dextrose, concentrated fruit juice, and honey.)
- If you drink alcohol, do so in moderation. The AHA recommends limiting alcohol to no more than 2 drinks per day for men and 1 drink per day for women.
Weight Reduction
People should aim for a BMI index of 18.5 - 24.9. Weight reduction is recommended for obese patients who have high blood pressure, high cholesterol levels, metabolic syndrome, or diabetes.
Some obese patients with coronary artery disease may consider having bariatric surgery (stomach bypass) to lose excess weight. The weight lost after surgery can help improve blood pressure, cholesterol, blood sugar and other factors associated with CAD.
Exercise
Everyone in normal health should do at least moderate physical activity for a minimum of 30 - 60 minutes on most, if not all, days of the week
Even low amounts of moderate or high intensity exercise (walking or jogging 12 miles a week) can help produce beneficial changes in cholesterol and lipid levels. However, more prolonged exercise is required to significantly change cholesterol levels, notably by increasing HDL ("good cholesterol"). Resistance (weight) training has also been associated with heart protection.
Click the icon to see an image of agina.
Your doctor needs to know if your activity causes any angina symptoms. Sudden strenuous exercise (especially snow shoveling) puts many people at risk for angina and heart attack. Patients with angina should never exercise shortly after eating. People with risk factors for heart disease should seek medical clearance and a detailed exercise prescription. And all people, including healthy individuals, should listen carefully to their bodies for signs of distress as they exercise.
Sexual Activity. Most patients with stable CAD can safely engage in sexual activity. Patients with severe heart disease should abstain from sex until their condition has stabilized. Exercise and cardiac rehabilitation can help lower the risks associated with sexual exertion.
PDE5 inhibitor drugs [sildenafil (Viagra), vardenafil (Levitra), tadalafil (Cialis), avanafil (Stendra)] are safe and helpful for most patients with stable CAD who have issues with erectile dysfunction. However, patients who take nitrate drugs in any form must never take PDE5 inhibitors.
Influenza Vaccination (Flu Shot)
Patients with CAD are considered at high risk for complications from influenza. People with CAD should get an annual flu shot.
Treatment
Lifestyle changes (such as weight control, exercise, and quitting smoking) are the first approach for all degrees of coronary artery disease. Depending on severity and individual conditions, patients may also need one or more medications, surgery, or both.
Medications. Many types of medications are used to treat angina and CAD. They include:
- Anti-platelet and anticoagulant drugs (used for preventing heart disease and preventing blood clots prior to surgery or after stent insertion)
- Beta blockers
- ACE inhibitors
- Nitrates
- Calcium channel blockers
Interventional Procedures and Surgery. Intervention is usually recommended for people who have:
- Unstable angina that does not respond promptly to medical treatment
- Severe recurrent episodes of angina that last more than 20 minutes
- Acute coronary syndrome
- Severe coronary artery disease (severe angina, multi-artery involvement, evidence of ischemia, or significant narrowing of left main coronary artery), particularly if abnormalities are evident in the left ventricle of the heart, the main pumping chamber
The two main surgical procedures for patients with coronary artery disease are:
- Coronary artery bypass grafting (commonly called bypass or CABG), which is usually reserved for patients with severe coronary artery disease.
- Percutaneous coronary intervention (commonly called angioplasty or PCI), usually with coronary artery stent placement. PCI is less invasive than CABG, but blood vessels can close up again (restenosis) so that patients require additional procedures.
The decision to choose angioplasty or coronary artery bypass depends on a patient’s individual profile, including the number and types of coronary arteries involved, the health stability, previous procedures, patient preference, and more.
Patients considering surgery should discuss all options and risks with their doctors. Guidelines recommend that patients with CAD discuss their treatment options with a medical team that includes both a cardiac surgeon (who performs CABG) and an interventional cardiologist (who performs PCI). No surgical procedure cures coronary artery disease, and patients must continue to rigorously maintain a healthy lifestyle and any necessary medications. For some patients, lifestyle changes and medications may be able to control the disease without surgery or angioplasty.
Medications
Anti-Platelet Drugs
Anti-clotting drugs that inhibit or break up blood clots are used at every stage of heart disease. They are generally classified as either anti-platelets or anticoagulants. Both anti-platelets and anticoagulants prevent blood clots from forming, but they work in different ways. Anti-platelets prevent blood platelets from sticking together. Anticoagulants are “blood thinners” that stop blood from clotting. Both of these therapies carry the risk of bleeding, which can lead to dangerous situations, including stroke.
For most patients with CAD, anti-platelet drugs are preferred over anticoagulants. Anticoagulants may be prescribed for patients with atrial fibrillation or prosthetic heart valves.
Current guidelines recommend that patients with CAD receive anti-platelet therapy with either aspirin or clopidgorel. Two newer anti-platelet drugs, Prasugrel (Effient) and ticagrelor (Brilinta), may be recommended for patients with acute coronary syndrome (unstable angina or early signs of heart attack) who have received a stent during PCI.
Aspirin. Aspirin is known as a nonsteroidal anti-inflammatory drug (NSAID). It stops blood platelets, which are major clotting factors, from sticking together to form a blood clot. Aspirin therapy is extremely beneficial for patients with coronary artery disease or history of stroke.
If you have been diagnosed with CAD, your doctor may recommend that you take a daily dose (from 75 – 162 mg) of aspirin. A daily dose of 81 mg is recommended for patients who have undergone PCI (angioplasty). Aspirin can reduce the risk of heart attack and ischemic stroke. However, prolonged use of aspirin can increase the risks for stomach bleeding. A doctor needs to consider a patient’s overall medical condition and risk factors for heart attack before recommending aspirin therapy.
A daily low-dose aspirin (75 - 81 mg) is usually the first choice for preventing heart disease or stroke in high-risk individuals. In general, daily low-dose aspirin is recommended for prevention of heart disease for the following people who have never had a heart attack or stroke:
- Women age 55 - 79. (Women who are younger than age 55 should not take aspirin for primary prevention.)
- Men age 45 - 79 years should take aspirin if the chances for preventing stroke or heart attack outweigh the risks of gastrointestinal bleeding. Men younger than age 45 should not take aspirin for primary prevention.
- For women and men age 80 years or older, it is not clear if the benefits of aspirin for heart protection outweigh the risks for bleeding.
Clopidogrel. Thienopyridines are anti-platelet drugs. Clopidogrel (Plavix, generic) is the standard thienopyridine for patients with CAD. Prasugrel (Effient) is a new thienopyridine that may be prescribed for patients with acute coronary syndrome.
For heart disease primary and secondary prevention, daily aspirin is generally the first choice. Clopidogrel is prescribed instead of aspirin for patients who are aspirin allergic or who cannot tolerate aspirin. For most patients, clopidogrel is not taken in combination with aspirin because the two drugs combined can increase the risk of bleeding.
Clopidogrel is also recommended for patients who are undergoing angioplasty. Patients who receive drug-coated stents require prolonged clopidogrel therapy. Patients having coronary bypass surgery should not take clopidogrel for at least 5 days prior to surgery because of a significant bleeding risk.
Thienopyridine anti-platelet drugs like clopidogrel can increase the risk for upper gastrointestinal bleeding, especially for patients who have pre-existing ulcers or other risk factors. For this reason, some doctors recommend that patients who are at high risk of gastrointestinal bleeding take a proton pump inhibitor (PPI) drug along with clopidogrel. PPI drugs help suppress gastric acid production, which in turn helps heal ulcers. However, PPI drugs can interfere with clopidogrel’s anti-platelet effects. Discuss with your doctor the risks and benefits of taking a PPI drug along with clopidogrel and whether this is right for you.
Beta Blockers
Beta blockers are useful for preventing angina attacks and reducing high blood pressure. They reduce the heart's oxygen demand by slowing the heart rate and lowering blood pressure. They can help reduce risk of death from heart disease and from heart surgeries, including PCI and coronary bypass.
Beta blockers are used or recommended in a number of situations:
- They are started in nearly all patients who have just had a heart attack or acute coronary syndrome.
- They are the drugs of choice for older patients with stable angina and may also be beneficial for people with silent ischemia. They are less useful for the treatment of Prinzmetal’s angina.
- They may be used alone or with other medications for management of rhythm disturbances or high blood pressure.
Beta blockers include propranolol (Inderal), carvedilol (Coreg), bisoprolol (Zebeta), acebutolol (Sectral), atenolol (Tenormin), labetalol (Normodyne, Trandate), metoprolol (Lopressor, Toprol-XL), and esmolol (Brevibloc). All of these drugs are available in generic form. A nasal spray form of propranolol may be helpful in reducing exercise-induced angina attacks.
Side Effects. Beta blocker side effects include fatigue, lethargy, vivid dreams and nightmares, depression, memory loss, and dizziness. They can lower HDL (“good”) cholesterol. Beta blockers are categorized as non-selective or selective. Non-selective beta blockers, such as carvedilol and propranolol, can narrow bronchial airways. These beta blockers should not be used by patients with asthma, emphysema, or chronic bronchitis.
PATIENTS SHOULD NEVER ABRUPTLY STOP TAKING THESE DRUGS. The sudden withdrawal of beta blockers can rapidly increase heart rate and blood pressure. The doctor may advise a patient to slowly decrease the dose before stopping completely.
Angiotensin Converting Enzyme (ACE) Inhibitors
Angiotensin converting enzyme (ACE) inhibitors are important heart-protective drugs, particularly for people with diabetes and high blood pressure. They reduce the production of angiotensin, a chemical that causes arteries to narrow, and so are commonly used to lower blood pressure. They may also reduce risk for heart attack, stroke, complications of diabetes, and death in patients at high risk for heart disease.
ACE inhibitors are indicated for most patients who have had heart attacks. They are particularly helpful for patients with coronary artery disease who also have diabetes or who have heart failure or left ventricular dysfunction (when the heart's main chamber does not pump as well as it should).
ACE inhibitors include captopril (Capoten, generic), ramipril (Altace, generic), enalapril (Vasotec, generic), quinapril (Accupril, generic), benazepril (Lotensin, generic), perindopril (Aceon, generic), and lisinopril (Prinivil, Zestril, generic).
Side Effects. Side effects of ACE inhibitors may include an irritating cough. More serious side effects are uncommon but may include excessive drops in blood pressure, allergic reactions, and high blood potassium levels. If you cannot tolerate the side effects of ACE inhibitors, your doctor may prescribe an angiotensin receptor blocker (ARB) as an alternative high blood pressure drug.
Nitrates
Nitrates have been used in the treatment of angina for over 100 years. These drugs release nitric oxide, thereby relaxing the smooth muscles in blood vessels. Nitrates are used primarily for control of angina symptoms. Many nitrate preparations are available. The most commonly used are nitroglycerin, isosorbide dinitrate, and isosorbide mononitrate. Nitrates can be absorbed from the gastrointestinal tract (oral tablet), skin (ointment or patch), or from under the tongue (sublingual tablet or spray).
Rapid Acting Nitrates. Rapid-acting nitrates are used to treat acute attacks. Nitroglycerin is the most widely used drug for this purpose. It can be administered under the tongue (sublingually or as a spray) or pocketed between the upper lip and gum (buccally) and can relieve angina within minutes. The procedure for taking nitroglycerin during an attack is as follows:
- At the onset of an angina attack, the patient administers one sublingual or buccal tablet or one metered dose of the spray.
- If the pain is not relieved within 5 minutes the patient takes a second dose; a third can be taken after another 5 minutes if symptoms persist.
- If pain continues after a total of three doses in 15 minutes, the patient should go immediately to the nearest emergency room.
Nitroglycerin is very unstable so its potency can be easily lost. Patients should take the following precautions:
- Keep no more than 100 tablets on hand, stored in their original container.
- When first opened, the cotton filler should be discarded, and the cap screwed on tightly immediately after each use.
- A supply should always be kept close at hand in case of an attack, with the rest kept in a cool dry place.
Intermediate to Long-Term Nitrates. Sublingual tablets of isosorbide dinitrate have a slower onset of action than nitroglycerin and are useful for preventing exercise angina. Ointments, skin patches, and oral tablets are used for longer-term prevention of angina attacks:
- Transdermal skin patches are applied in the morning to any hair- or injury-free area on the chest, back, stomach, thigh, or upper arm. Hands should be washed after each patch or ointment application, and sites of application should be rotated to avoid skin irritation.
- Nitroglycerin ointment is applied by measuring out an even amount on an applicator paper and then placing, not rubbing or massaging, it on the chest, stomach, or thigh. Any ointment that remains from the previous application should be removed.
Long-acting forms may lose their effectiveness over time, so doctors generally schedule nitrate-free breaks to prevent tolerance.
Side Effects. Nitrates can have many side effects, some of which can be serious.
Common side effects of nitrates include headaches, dizziness, nausea and vomiting, blurred vision, fast heartbeat, sweating, and flushing on the face and neck. Low blood pressure and dizziness can be relieved by lying down with the legs elevated. These effects are significantly worsened by alcohol, beta blockers, calcium channel blockers, and certain antidepressants. Patients who take nitrates in any form cannot take medications for erectile dysfunction, such as sildenafil (Viagra), vardenafil (Levitra), tadalafil (Cialis), and avanafil (Stendra). The doctor may prescribe medicines to lessen these side effects. Patients should contact their doctor if these side effects are persistent or severe.
Serious side effects requiring immediate medical help include fever, joint or chest pain, sore throat, skin rash (especially on the face), unusual bleeding or bruising, weight gain, and swelling of the ankles.
Withdrawal. Withdrawal from nitrates should be gradual. Abrupt termination may cause angina attacks.
Calcium Channel Blockers (CCBs)
Calcium channel blockers reduce heart rate and slightly dilate the blood vessels of the heart, thereby decreasing oxygen demand and increasing oxygen supply. They also reduce blood pressure. CCBs vary chemically, however, and although some are helpful, others may even be dangerous for certain patients with CAD.
Click the icon to see an image of heart arteries.
- Long-acting nifedipine (Adalat, Procardia, generic) and nisoldipine (Sular, generic) and newer CCBs, such as amlodipine (Norvasc, generic) and nicardipine (Cardene, generic), may be beneficial for some patients with angina. They can be considered alone for patients who cannot tolerate beta blockers, but may provide the best results when used in combination with a beta blocker. Studies suggest that they reduce the need for repeat angioplasties. Their effects on other outcomes, including mortality rates and heart attack, are less clear.
- Short-acting CCBs, including short-acting forms of verapamil, diltiazem, nifedipine, and nicardipine, are helpful for many patients with Prinzmetal's angina. However, short-acting forms of certain CCBs, such as nifedipine and nisoldipine, have been associated with severe and even dangerous side effects, including an increase in heart attacks and sudden death in some patients with unstable angina. They also increase the risk for adverse effects in patients with stable angina. Short-acting CCBs are, therefore, not used for stable or unstable angina.
There is no strong evidence that any calcium channel blockers improve survival rates. Overdose can cause dangerously low blood pressure and slow heart beats. Patients with heart failure have a higher risk for death with these drugs and should not take them. No one taking any calcium channel blocker should withdraw abruptly because such action could dangerously increase the risk of high blood pressure. Note: Grapefruit and Seville oranges boost the effects of certain CCBs, sometimes to toxic levels. (Regular oranges do not appear to pose any hazard.)
Other Drugs
Ranolazine (Ranexa) is used to treat chronic angina in patients who have not responded to other angina drugs. Ranolazine is taken in combination with amlodipine, beta blockers, or nitrates.
Surgery
Angioplasty and Stents
Angioplasty, also called percutaneous coronary intervention (PCI), involves procedures such as percutaneous transluminal coronary angioplasty (PTCA) that help open the blocked artery.
Angioplasty can help reduce the frequency of angina attacks for patients who have not been helped by drug therapy. It is commonly recommended for patients who have critically blocked arteries or have already had a recent, acute heart attack. Angioplasty can also help improve survival and prevent heart attacks in patients with acute coronary syndrome (ACS). However, doctors have been uncertain about angioplasty's benefits for survival and heart attack prevention in lower-risk patients with stable coronary artery disease.
Angioplasty works no better than standard heart medication (drugs to control blood pressure, lower cholesterol, and prevent blood clots) in preventing heart attack, stroke, and hospitalization in patients with stable coronary artery disease. Doctors now recommend angioplasty only for patients who have severe heart disease. For patients with stable heart disease, drug therapy may be sufficient enough treatment and allow them to safely defer having surgery.

Click the icon to see an animation about percutaneous coronary intervention.
Procedure. A typical angioplasty procedure follows these steps:
- The cardiologist threads a narrow catheter (a tube) containing a catheter from the groin area into the blocked vessel.
- The doctor opens the blocked vessel using balloon angioplasty, in which the surgeon passes a tiny deflated balloon through the catheter to the vessel.
- The balloon is inflated to compress the plaque against the walls of the artery, flattening it out so that blood can once again flow through the blood vessel freely.
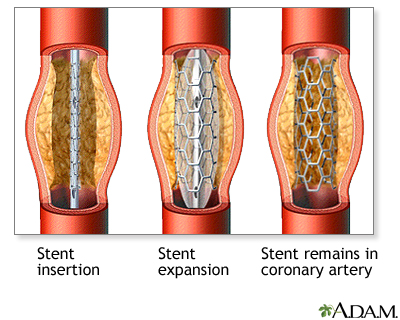
- To keep the artery open afterwards, doctors use a device called a coronary stent, an expandable metal mesh tube that is implanted during angioplasty at the site of the blockage. (In some cases, a stent may be used as the initial opening device instead of balloon angioplasty.) The stent may be bare metal or it may be coated with a drug that slowly releases medication.
- Once in place, the stent pushes against the wall of the artery to keep it open.

Click the icon to see an animation about angioplasty.
Complications occur in about 10% of patients (about 80% of them happening within the first day). Success rates are better in hospital settings with experienced teams and backup.

Click the icon to see a series about angioplasty.
Recuperation and Complications. Angioplasty is less invasive than bypass surgery, requiring only one night in the hospital. Recuperation takes about a week. Chest pain after the procedure is very common and usually due to problems other than ischemia. Mild chest pain is even more common when a stent is used, possibly because the artery is stretched.
The most important short- and long-term complication of angioplasty is narrowing or reclosure (restenosis) of the artery, which can lead to heart attack if not treated with a repeat procedure. Stenting, anti-clotting drugs, and other advances have significantly helped prevent reclosure and reduce heart attack rates. Nevertheless, a repeat procedure is still needed to restore the opening in 10 - 15% of patients who have stents.
Drug-Coated Stents. Stents coated with the drugs sirolimus (Rapamune) or paclitaxel (Taxol) have been increasingly used in the last several years. Drug-eluting stents (as they are also called) can help prevent restenosis. However, because drug-eluting stents reduce arterial tissue growth, they can increase the risks of blood clots.
Recent studies indicate that drug-eluting stents are safe and effective for patients with coronary artery disease when they are used for FDA-approved indications. Some studies have indicated that problems may arise when these stents are used for “off-label” purposes in patients with more complicated health problems, although other studies have found no increased risks. There is still some concern that all stents (both bare metal and drug eluting) may be used too frequently for patients who may be better served by drugs or bypass surgery.
It is very important that all patients who have drug-eluting stents take aspirin and clopidogrel for at least 1 year after the stent is inserted to reduce the risk of blood clots. For patients undergoing PCI who have acute coronary syndrome, two newer antiplatelet drugs – prasugrel (Effient) or ticagrelor (Brilinta) – may be options. These drugs, like aspirin, help prevent blood platelets from clumping together. It is important that patients who have drug-eluting stents take both aspirin and another anti-platelet drug. If for some reason patients cannot stick to a dual anti-platelet regimen, they should receive a bare metal stent instead of a drug-eluting stent.
Coronary Artery Bypass Graft Surgery
Coronary artery bypass graft surgery (CABG) is an alternative to angioplasty for many patients with severe coronary artery disease, but it is a very invasive open-heart surgical procedure.
Minimally invasive coronary artery bypass surgery (MIDCAB), also called “keyhole heart surgery,” may be an option for some patients. It uses various techniques, including endoscopy or robotic-assisted approaches. Unlike standard CABG, with MIDCAB patients do not have their heart stopped and do not have to be put on a heart-lung machine during the procedure. In MIDCAB, the surgeon uses a smaller incision on the left side of the chest. CABG requires a longer incision down the center of the chest.
In a traditional CABG procedure:

Click the icon to see an animation about coronary artery bypass grafting.

Click the icon to see an image of heart bypass surgery.
- The chest is opened, and the blood is rerouted through a lung-heart machine.
- The heart is stopped during the procedure.
- Blood vessel grafts are taken from arteries or veins in the chest wall or other areas of the body. The grafts are transplanted in front of and beyond the blocked arteries, so the blood flows through the new vessels around the blockage. Patients may require one, two, or three grafts (or more) depending on the number of coronary arteries that are blocked.
- In general, patients with triple bypass procedures stay in the hospital for 5 or 6 days. Those with one-vessel bypass may be able to go home in 3 days.

Click the icon to see a series about heart bypass surgery.
Complications. Complications are generally rare but can include bleeding, infections, heart attack, and stroke. Finding a surgeon who performs at least 100 of the procedures a year helps reduce the risk for complications.
Blood clots may form in the new graft, closing it up or narrowing the treated vessel over time. Therapy with aspirin and other anti-clotting drugs help keep the graft open and working properly.
Recuperation and Rehabilitation. After leaving the hospital, patients should have cardiac rehabilitation. Guidelines recommend that doctors refer patients who have had CABG or PCI to a comprehensive outpatient cardiac rehabilitation program. Rehabilitation includes education about healthy diet and lifestyle choices, as well as exercise training to rebuild strength and stamina.
Resources
- www.nhlbi.nih.gov -- National Heart, Lung, and Blood Institute
- www.heart.org -- American Heart Association
- www.acc.org -- American College of Cardiology
References
Abraham NS, Hlatky MA, Antman EM, Bhatt DL, Bjorkman DJ, Clark CB, et al. ACCF/ACG/AHA 2010 Expert Consensus Document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation. 2010 Dec 14;122(24):2619-33. Epub 2010 Nov 8.
Bhatt DL, Cryer BL, Contant CF, Cohen M, Lanas A, Schnitzer TJ, et al. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med. 2010 Nov 11;363(20):1909-17. Epub 2010 Oct 6.
Bluemke DA, Achenbach S, Budoff M, Gerber TC, Gersh B, Hillis LD, et al. Noninvasive coronary artery imaging: magnetic resonance angiography and multidetector computed tomography angiography: a scientific statement from the American Heart Association committee on cardiovascular imaging and intervention of the council on cardiovascular radiology and intervention, and the councils on clinical cardiology and cardiovascular disease in the young. Circulation. 2008 Jul 29;118(5):586-606. Epub 2008 Jun 27.
Boden WE, O'Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007 Mar 26; [Epub ahead of print]
Bravata DM, Gienger AL, McDonald KM, Sundaram V, Perez MV, Varghese R, et al. Systematic review: the comparative effectiveness of percutaneous coronary interventions and coronary artery bypass graft surgery. Ann Intern Med. 2007 Nov 20;147(10):703-16. Epub 2007 Oct 15.
Drozda J Jr, Messer JV, Spertus J, Abramowitz B, Alexander K, Beam CT, et al. ACCF/AHA/AMA-PCPI 2011 performance measures for adults with coronary artery disease and hypertension: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures and the American Medical Association-Physician Consortium for Performance Improvement. J Am Coll Cardiol. 2011 Jul 12;58(3):316-36. Epub 2011 Jun 14.
Ebbing M, Bleie O, Ueland PM, Nordrehaug JE, Nilsen DW, Vollset SE, et al. Mortality and cardiovascular events in patients treated with homocysteine-lowering B vitamins after coronary angiography: a randomized controlled trial. JAMA. 2008 Aug 20;300.
Eisenstein EL, Anstrom KJ, Kong DF, Shaw LK, Tuttle RH, Mark DB, et al. Clopidogrel use and long-term clinical outcomes after drug-eluting stent implantation. JAMA. 2007 Jan 10;297(2):159-68. Epub 2006 Dec 5.
Fraker TD Jr, Fihn SD, Gibbons RJ, Abrams J, Chatterjee K, Daley J, et al. 2007 chronic angina focused update of the ACC/AHA 2002 Guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 Guidelines for the management of patients with chronic stable angina. Circulation. 2007 Dec 4;116(23):2762-72. Epub 2007 Nov 12.
Gaziano M, Ridker PM, Libby P. Primary and secondary prevention of coronary heart disease. In: Bonow RO, Mann DL, Zipes DP, Libby P, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 9th ed. Saunders; 2012:chap 49.
Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010 Dec 21;122(25):e584-636. Epub 2010 Nov 15.
Grines CL, Bonow RO, Casey DE Jr, Gardner TJ, Lockhart PB, Moliterno DJ, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. Circulation. 2007 Feb 13;115(6):813-8. Epub 2007 Jan 15.
Hemingway H, Langenberg C, Damant J, Frost C, Pyörälä K, Barrett-Connor E. Prevalence of angina in women versus men: a systematic review and meta-analysis of international variations across 31 countries. Circulation. 2008 Mar 25;117(12):1526-36. Epub 2008 Mar 17.
Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, et al. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011 Dec 6;58(24):e123-210. Epub 2011 Nov 7.
Kaiser C, Galatius S, Erne P, Eberli F, Alber H, Rickli H, et al. Drug-eluting versus bare-metal stents in large coronary arteries. N Engl J Med. 2010 Dec 9;363(24):2310-9. Epub 2010 Nov 16.
Kirtane AJ, Gupta A, Iyengar S, Moses JW, Leon MB, Applegate R, et al. Safety and efficacy of drug-eluting and bare metal stents: comprehensive meta-analysis of randomized trials and observational studies. Circulation. 2009 Jun 30;119(25):3198-206. Epub 2009 Jun 15.
Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011 Dec 6;58(24):e44-122. Epub 2011 Nov 7.
Levine GN, Steinke EE, Bakaeen FG, Bozkurt B, Cheitlin MD, Conti JB, et al. Sexual activity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2012 Feb 28;125(8):1058-72. Epub 2012 Jan 19.
Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, et al. Effectiveness-Based Guidelines for the Prevention of Cardiovascular Disease in Women--2011 Update: A Guideline From the American Heart Association. Circulation. 2011 Feb 16. [Epub ahead of print]
Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009 Mar 5;360(10):961-72. Epub 2009 Feb 18.
Smith SC Jr, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation endorsed by the World Heart Federation and the Preventive Cardiovascular Nurses Association. J Am Coll Cardiol. 2011 Nov 29;58(23):2432-46. Epub 2011 Nov 3.
Trikalinos TA, Alsheikh-Ali AA, Tatsioni A, Nallamothu BK, Kent DM. Percutaneous coronary interventions for non-acute coronary artery disease: a quantitative 20-year synopsis and a network meta-analysis. Lancet. 2009 Mar 14;373(9667):911-8.
Vandvik PO, Lincoff AM, Gore JM, Gutterman DD, Sonnenberg FA, Alonso-Coello P, et al. Primary and secondary prevention of cardiovascular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012 Feb;141(2 Suppl):e637S-68S.
Weintraub WS, Spertus JA, Kolm P, Maron DJ, Zhang Z, Jurkovitz C, et al. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med. 2008 Aug 14;359(7):677-87.
US Preventive Services Task Force. Aspirin for the prevention of cardiovascular disease: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009 Mar 17;150(6):396-404.
U.S. Preventive Services Task Force. Using nontraditional risk factors in coronary heart disease risk assessment: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009 Oct 6;151(7):474-82.
|
Review Date:
5/24/2012 Reviewed By: Harvey Simon, MD, Editor-in-Chief, Associate Professor of Medicine, Harvard Medical School; Physician, Massachusetts General Hospital. Also reviewed by David Zieve, MD, MHA, Medical Director, A.D.A.M., Inc. |